Results of the ADEA CDE Education Review Survey

Introduction
In 2020 the Australian Diabetes Educators Association (ADEA) began conducting an end-to-end education review to re-examine the education a Credentialled Diabetes Educator (CDE) requires. All components of the education pathway, including the Graduate Certificate of Diabetes Education (GradCertDE) and the initial and recredentialling process and required activities are being considered, to assess whether the current model still meets the education needs of CDEs, particularly as the role of a CDE continues to evolve.
The purpose of this review is to ensure standardised and contemporary education for the diabetes education workforce of the future, to meet the needs of people with diabetes in Australia and ensure CDEs are well positioned and recognised as diabetes specialists in the health system.
A significant part of this review was the CDE Education Review Survey conducted in August 2020, to obtain perceptions among the ADEA membership and key stakeholder groups concerning CDE education. This article provides an overview of the major findings of the survey.
Methods
The CDE Education Review Survey was conducted online with the aim of capturing a range of stakeholders including CDEs, diabetes educators (DE), employers and supervisors of CDEs and DEs, and current students, recent graduates, course coordinators, lecturers, and educators of the GradCertDE courses.
The questions related to the GradCertDE, National Competencies for CDEs, their role and scope of practice, initial credentialling and recredentialling. Quantitative data was collected, and likert-scale and open-ended questions were used to gather more detailed information, experiences, and suggestions. The data was analysed using SPSS Statistics 25 and content analysis was applied to open-ended response questions to identify themes. Comparison between responses from different stakeholder groups was also conducted e.g., students vs CDEs.
Participants were recruited via email, social media and the ADEA newsletter. Demographic data was collected to ensure the survey was representative of ADEA’s membership and that a range of stakeholder views was captured. Overall participation was representative regarding the distribution of CDE status, primary discipline, state, geographical location, and employment setting.
In total, 333 people attempted the online survey. Of those, 14 were excluded due to incomplete surveys, resulting in a final data set of 319 completed surveys. Of the 319 participants, 254 were CDEs, 29 were current students, 20 were graduates of the GradCertDE and currently working towards credentialling, and 14 were DEs without the CDE credential.
Participants were also asked to identify themselves in any of the additional stakeholder groups listed. Of the 319 participants, 37 were supervisors, employers or managers of CDEs or DEs, 14 were course coordinators or educators for the GradCertDE, 15 were either ADEA Course Accreditation and Standards of Practice (CASP), credentialling, or clinical practice committee members, with the remaining 253 not identifying themselves in any of these groups.
Results
Participants were asked a series of questions concerning aspects of CDE education including postgraduate study, the credentialling program, the National Competencies for CDEs, and CDE role and scope of practice.
Postgraduate Study
When asked to rank how prepared graduates of the GradCertDE are to take on the role of a DE, overall, just over half of all respondents (54%) felt they were somewhat or well prepared, whereas 37% thought they were somewhat or very unprepared (Figure 1).
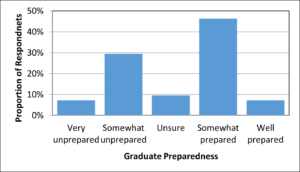
Figure 1. Survey respondents perceived preparedness of graduates of the GradCertDE for the role of a DE
When asked if respondents identified any practical skills in which graduates are lacking entry level experience, competence or confidence after completing the GradCertDE, 55% answered ‘Yes’, 25% were ‘Unsure’, 11% answered ‘No’ and 9% were unable to say because they had not yet completed the GradCertDE.
Most survey respondents felt that the theoretical component of the GradCertDE was comprehensive. However, the practical skills reported to be lacking most frequently among graduates were the use of technology and devices, including blood glucose meters, insulin pens and continuous glucose monitoring (CGM). The second most reported deficit was skills in client assessment, management of complex clients and problem-solving. Also frequently reported was the management of medication, consultation and interviewing skills, person-centred care, health behaviour and coaching skills.
The survey asked what level of qualification was most appropriate to learn the required knowledge and skills of a DE. Overall, the Graduate Certificate level (4 units) was selected by 36%, the Graduate Diploma level (8 units) 47%, the Masters level (12 units) received 7%, while 10% of respondents were unsure. This question was further analysed by stakeholder group (Figure 2). The majority of those in the supervisor/employer and course coordinator/educator groups and more than half (54%) of CDEs who participated in the survey indicated the Graduate Diploma was the most appropriate qualification for diabetes education.
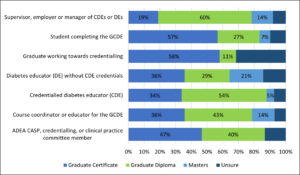
Figure 2. Perception of Appropriate qualification level for diabetes education knowledge and skills by stakeholder group
A series of questions were asked about the clinical placement requirement, which is a 40-hour clinical placement and 20 hours of other practical experience (e.g., simulation, workshops, professional development activity). In preparing students with the practical skills for a DE role, most participants (70%), indicated the current requirement for clinical placement is not long enough (Figure 3).
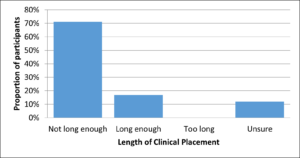
Figure 3. Adequacy of current clinical placement requirement (40-hour placement + 20 hours of other practical experience)
Participants were asked to suggest how the GradCertDE course could better prepare graduates for the role of a DE. Key themes included:
- Longer and more varied placement
- More practical skills training
- More case-studies/real life scenarios in the course
- More specific scope of practice learning
- More education on technology
- Opportunities for mentoring during the course
- Have a buddy system or supervised practice
Credentialling
Participants were asked to rate the extent to which they agreed or disagreed with a series of statements concerning the CDE initial credentialling program (Figure 4). Overall, 43% agreed that the credentialling process was easy for prospective CDEs to navigate and complete, 90% agreed that the mentoring program is an important component of initial credentialling, and 50% agreed the initial credentialling program meets the expectations of prospective CDEs and supports a high standard of CDEs entering the workforce.

Figure 4. Extent to which respondents agree/disagree with the CDE credentialling statements
Participants were asked to offer suggestions for how the credentialling program could be improved to better prepare and support DEs becoming CDEs. Most comments were related to improving the process of credentialling, including navigation and function of the ADEA website, documentation, providing more information about the process and requirements, and making it less complex and time consuming.
Participants were asked to rate the extent to which they agreed or disagreed with a series of statements concerning the CDE recredentialling program (Figure 5). Overall, 30% disagreed and another 30% were unsure if there are opportunities to advance practice as a CDE, 45% disagreed and another 30% were unsure if a clear career progression pathway exists for CDEs, while 23% disagreed and 32% were unsure if recredentialling supported career development.
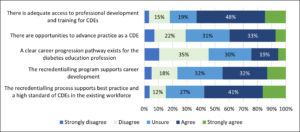
Figure 5. Extent to which respondents agree/disagree with the continuing professional development and career development statements
In response to the question ‘If additional or other education is required to adequately prepare DEs for CDE status, is it important to upskill current CDEs so all are qualified the same?’, 32% of participants answered ‘yes’, 27% answered ‘unsure’ and 41% answered ‘no’. Those that answered ‘yes’ were asked to provide any suggestions for how current CDEs might gain this additional learning. The most common suggestion was to upskill current CDEs through ADEA-led education activities such as webinars, workshops, or online modules that could be included in the recredentialling process. Others suggested an assessment or mentoring program.
National Competencies for CDEs
When asked about the National Competencies for CDEs, 60% agreed the current document captures required competencies, major work roles and purpose and function of a CDE (Figure 6). However, some respondents felt they needed to be more specific to the various primary disciplines and that they don’t adequately outline or describe the scope of all disciplines. A lack of direction in the competencies concerning insulin administration and adjustment was raised by some, who commented that greater direction is needed concerning who is trained and authorised to practice in this area and suggested clearer guidance through the competencies. Some commented on the need for the competencies to recognise different levels of expertise.
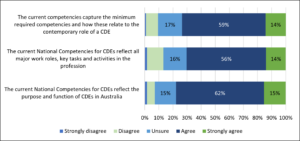
Figure 6. Extent to which respondents agreed or disagreed with the National Competencies for CDEs statements
Scope of Practice
Participants were asked to indicate whether they agreed or disagreed with a series of statements concerning the role and scope of practice of a CDE (Figure 7). Overall, 60% disagreed that the scope of practice of a CDE is clear to people with diabetes, 40% disagreed that the scope of practice of a CDE is clear among the existing workforce, and 32% disagreed scope of practice is clear among new graduates.
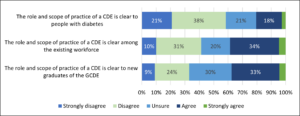
Figure 7. Extent to which participants disagreed or agree with the statements about Role and Scope of Practice
Participants were then asked to describe any ambiguities they perceive in the role boundaries and scope of practice of CDEs. This was with respect to the various primary disciplines, the evolving nature of the CDE role and the different clinical contexts in which CDEs work. The themes identified outlined feelings among the existing CDE workforce concerning uncertainty of their own scope of practice and the scope of practice of others, role boundaries and primary discipline, varying levels of skill and authority.
Survey participants were asked their views on what could be done to clarify and/or make consistent the role boundaries and scope of practice of CDEs (Table 1). Two thirds believed ensuring standardised education across tertiary institutions and providing opportunities to learn role boundaries and scope of practice could assist. Incorporating role boundaries and scope of practice into the GradCertDE to a greater extent as well as ensuring consistency across clinical placements was chosen by 60% of participants. Additional suggestions included differentiating an advanced/extended level of practice and more rigorous assessment during initial credentialling and recredentialling.
Table 1. What could be done to clarify and/or make consistent the role boundaries and scope of practice of CDEs?
| What could be done to clarify and/or make consistent the role boundaries and scope of practice of CDEs? | Proportion who selected ‘Yes’ | Number |
| Ensure standardised education across institutions | 65.8% | 196 |
| Provide opportunities to learn the role boundaries and scope of practice external to the graduate certificate e.g., online modules, workshops | 64.1% | 191 |
| Incorporate role boundaries and scope of practice into the curriculum/course work to a greater extent | 60.7% | 181 |
| Ensure consistency in access to learning and competency development during clinical placements | 58.4% | 174 |
| Enhance ADEA guidelines concerning role and scope of practice | 56.7% | 169 |
| Ensure standardised education across all primary disciplines | 46.6% | 139 |
| Other | 12.8% | 38 |
| Unsure | 4% | 12 |
The Value of a CDE
A theme throughout the results of the survey was the value of a CDE. Several CDEs commented that they find their work very rewarding and indicated their motivation for pursuing study in diabetes education was to increase knowledge and skills to better support people with diabetes. However, many respondents felt that the value of the CDE credential and specialist knowledge was often not recognised. This related to postgraduate study, credentialling, scope of practice, job opportunities and recognition in the health system. Some of the suggestions made previously, such as clarifying scope of practice, recognising advanced practice, shifting to a higher qualification for CDEs, and standardising and assessing clinical competence, as well as advocacy for CDEs in the health system, were suggested as ways of improving the perceived value of a CDE.
Conclusion
The CDE Education Review Survey highlights the need for greater education and the opportunity to apply practical CDE skills, greater assessment of competence, and further mentoring and supervision opportunities. Issues of scope of practice, standardised education and competence, recognition of advanced practice and the perceived value of a CDE were also emphasised.
These key findings were reviewed by the CDE Education Review Expert Reference Group, Graduate Certificate in Diabetes Education Course Coordinators, the ADEA Course Accreditation and Standards of Practice Committee and ADEA Credentialling Committee. In consultation with these committees, recommendations for the second phase of the education review were developed. The recommendations, to be completed over the next 12 months, include reviewing CDE scope of practice and competency standards, to research the implications of changes to the education pathway, and to develop ADEA programs to support or deliver CDE education to a greater capacity.
Through the completion of these recommendations and further consultation with the key committees above, the CDE education and credentialling pathway will be re-shaped accordingly, toward ensuring CDEs are equipped to best support people with diabetes and are positioned as diabetes education specialists into the future.
Acknowledgements
ADEA would like to acknowledge Dr Virginia Hagger (Deakin University) and Dr Sheri Cooper (Southern Cross University) for their ongoing assistance with this project. ADEA would also like to acknowledge the CDE Education Review Expert Reference Group, ADEA Credentialling Committee, ADEA CASP Committee and Graduate Certificate of Diabetes Education Course Coordinators for their contributions to this project to date.