Nutrition in Wound Healing for Adults with Diabetes: A Practice Update
Introduction
People with diabetes have a higher prevalence of wounds due to suboptimally managed glucose levels, ischaemia, neuropathy, pressure, friction, infection, nutritional status or a combination of these1, 2. Rates of diabetes are expected to rise alongside an ageing population and increased incidence of obesity, with the projected global prevalence expected to reach 4.4% by 20363. As the number of people with diabetes rises, so too will the number of associated wounds that health care professionals will be expected to manage. Currently chronic ulcers/wounds cost the Australian health system approximately $2.86 billion/year4, with most of these being managed in general practice settings5.
Definitions
An ulcer present for more than three months is defined as a chronic ulcer6, while a chronic wound is defined as one which persists for more than six weeks or recurs frequently7.
The Wound Healing Society classifies ulcers into four groups: pressure ulcer, diabetic ulcer, venous ulcer and arterial insufficiency ulcer8. Alternatively, ulcers can be classified based on their cause including vascular (venous, arterial or mixed), neuropathic (diabetes, tabes, syringomyelia), metabolic (diabetes, gout, prolidase deficiency), trauma-related (pressure, injury, burns), infection-related (bacterial, fungal, protozoan), tumours (basal or squamous cell carcinomas); haemotological; pyoderma, panniculitis and hypertensive ulcers6.
Pressure ulcers occur when capillary blood flow is cut off from the tissue, from inside to outside9. They are directly caused by pressure, friction, shear, immobility, loss of sensation or combined pathology10. Indirect causes include poor nutrition, mobility problems, health conditions (e.g. diabetes, renal or cardiovascular disease, incontinence, ageing skin and mental health conditions)10. They generally occur in the coccyx, scapula, greater trocanter, occiput, elbows, heels and knees9, 10.
Diabetes-related foot ulcers generally occur on the plantar surface of the foot. They are caused by suboptimally managed diabetes, arterial insufficiency, peripheral neuropathy or when the calf-pump mechanism fails due to obstruction (Deep Vein Thrombosis (DVT) or extraluminal masses), regurgitation (valve weakness), venous incompetence (proximal DVT), vein weakness (primary varicose vein syndrome) or muscle failure (ankle trauma or surgical fusion)11-13.
Venous leg ulcers, the most common type of leg ulceration in the lower limb, occur as a result of venous insufficiency, venous hypertension and/or valve and calf muscle pump failures6, 12, 13. These are usually chronic and differ from neuropathic and arterial ulcers14.
Arterial ulcers are the second most common type of lower extremity ulcers and develop as a result of insufficient perfusion and oxygenation to the dermis or due to arterial ischaemia/occlusion which can likely result in limb loss12, 13.
Neurotrophic foot ulcers are due to peripheral neuropathy resulting in loss of sensation12, 15. Inadequate care (not wearing footwear/inappropriate footwear, not inspecting feet for dryness, cracks, injuries, calluses, not keeping the feet clean) in diabetic neuropathy can trigger new wounds due to loss of sensation/pain12, 13, 16.
Factors affecting wound management
There are several intrinsic and extrinsic factors that affect wound management17, 18. They include:
- type and location of wound1
- duration of the wound19
- the type of tissue involved1
- whether or not there is inflammation or infection1
- the level of moisture/hydration of the wound1
- person associated factors such as weight, hydration and nutrition status, exercise, glycaemic management, smoking1, 20
- other metabolic management and psycho-social support21
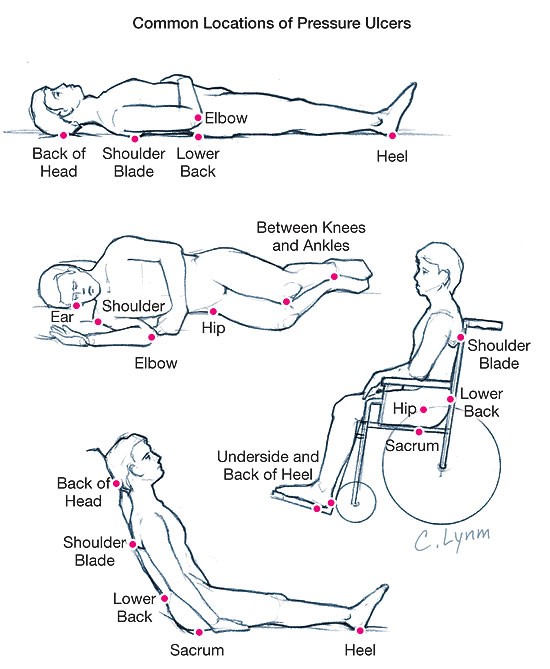
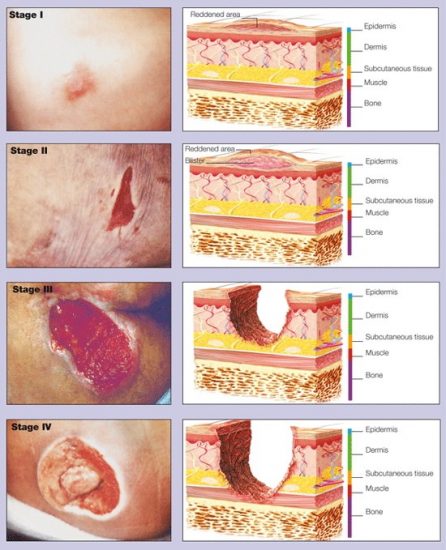
Figure 1. Reproduced with permission from Pressure ulcers, JAMA, January 8, 2003: Vol 289, No.2
The relationship between nutritional status and wound healing has been well researched, but it is not commonly considered in practice. Ongoing chronic wounds deplete lean body mass and affect mobility, pain and quality of life, particularly in the elderly22. Most published studies do not provide details of populations studied, the nature of the wounds (aetiology, stage of wound, etc), anthropometry or details of diet or nutrient intake23, 24. While a number of studies use oral nutrition supplements, enteral or parenteral nutrition, they appear to consider them as a single nutrition entity rather than the combined complex nutritional therapy that they can provide23-25. Moisture, mobility, sensory perception and activity are potential confounders in these studies23.
Nutrition in wound care is multifaceted as it involves different nutrients in various roles and stages of wound healing16, 26, 27. Immune function, wound tensile strength, and collagen synthesis are all influenced by nutrition26, 27. Some nutrients are required only in situations of deficiency, while others are conditionally essential16, 27, 28. Adequate quantities of all nutrients are necessary and have a therapeutic role at the cellular/extracellular level25, 27. There is an important place for a complete diet in wound care, with all nutrients being considered14, 27.
Phases of wound healing
The wound healing process involves different nutrients in different phases of wound healing16, 26, 28. The first phase is haemostasis which starts at the time of injury and lasts several hours26, 28, 29. During this phase there is formation of platelet plug and coagulation through vascular spasm18, 26, 29. The inflammatory phase begins at the time of injury and may last up to six days, when there is proliferation of metabolic mediators and a fibrin clot forms as a protective barrier for haemostasis16, 18, 26, 28-30. The next phase is the proliferative phase which starts three to five days after injury and may last up to three weeks16, 18, 26-29. During this phase fibroblast formation, angiogenesis, epithelialisation and collagen cross linking result in wound contraction16, 18, 26-31. This is followed by the remodelling phase approximately two weeks post injury, which can last up to two years18, 26-29. Collagen maturation and stabilisation during this phase results in wound tensile strength and scar formation26-30.
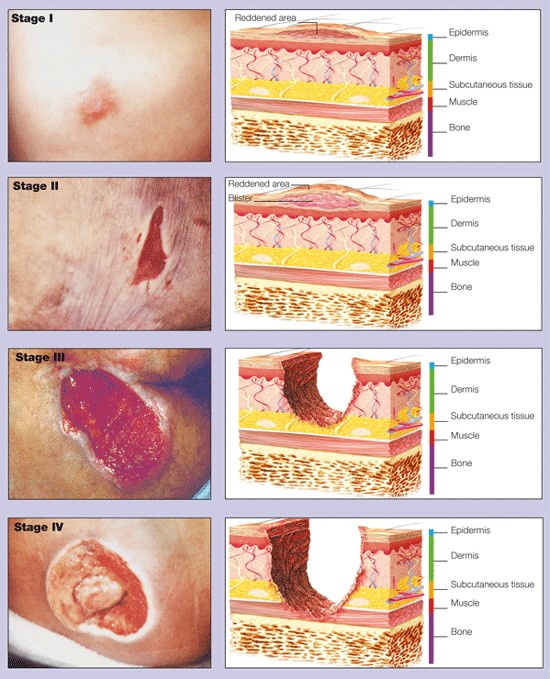
Figure 2. The NPUAP of pressure ulcer stages
Reproduced with permission from Ovid: How to assess pressure ulcers. Nursing Made Incredibly Easy!.7(6):20-25, November/December 2009. DOI:10.1097/01.NME.0000363319.70905.96
Role of nutrition in wound healing
The protracted nature of the wound healing process underscores the need for wound prevention, preparation (as in surgical) and treatment of acute and chronic wounds16, 30. Nutritional risk factors that delay/impair wound healing include malnutrition (which could include under-nutrition, over-nutrition and nutrient deficiencies)14, 25-28, 32-34, loss of appetite, dysgeusia, anosmia, inability to feed oneself, poor dental health, inadequate or excessive intake of macro and micronutrients and poor hydration16, 25-27, 30. In addition, delayed treatment, advancing age, stress, memory impairment, alcoholism and smoking, medication side effects, medical, psychological, physiological, physical, social and economic difficulties can often compound the problem16, 25-30.
Clinical markers are more commonly used than diagnostic markers in determining malnutrition32. Diagnostic markers of malnutrition are confounded by chronic infection or inflammation, other protein losing enteropathies, altered hepatic function and altered fluid status/shifts16, 26-28, 33. Checking Body Mass Index, C-reactive protein, albumin and pre-albumin levels have been suggested to monitor malnutrition status in people with wounds26-28, 33, 35.
Nutrition interventions should be individualised based on current body weight, age, multi-morbidities, activity level, stage of wound, severity, and number of wounds16, 26-28, 30. Nutrition support in wound healing should meet the increased energy and protein needs27, 33. Macronutrients such as carbohydrates, proteins, fats and their distribution; micronutrients such as vitamins A,D,E,K and C, minerals such as iron and zinc, and hydration all play a vital role in wound healing16, 25-28, 30, 33-36.
Role of nutrients
There is an increased need for energy in wound healing to promote anabolism and reverse catabolism35. Energy requirements for adults are around 30-35kcals/kg or 40cals/kg if underweight16, while older Australians need around 20-25kcals/kg 22.
Carbohydrates are an essential component of immunological, hormonal, enzymatic function and cell structure16, 22. They trigger insulin production which is useful in the proliferative phase as it is anabolic16. However, hyperglycaemia due to excess intake of carbohydrates (in diabetes) increases the risk of infectious complications and decreases granulocyte function16. Besides diabetes-induced hyperglycaemia, blood glucose can be elevated due to use of steroids, antibiotics, dextrose infusion in people without diabetes, infections and other physiological stressors increasing cortisol levels16. A diet with lower glycaemic index carbohydrate choices helps to manage blood glucose levels, but this is also dependent on its distribution across the day, meal combinations and several other factors. A meal plan with 40-50% carbohydrates is recommended22, 26, 32. Grains, starchy vegetables, fruit and legumes are the main sources of carbohydrates in the diet28, 35.
Proteins are essential for tissue growth, repair and regeneration thus vital for wound healing. Proteins provide amino acids and inadequate intake results in lean body mass degradation, increased skin fragility, decreased immune function and decreased reserve capacity due to microangiopathy, thus delaying wound healing and recovery16, 18, 22, 25-28, 30, 32-35. Essential amino acids are building blocks of cells, extracellular matrix and granulation tissue proteins37. If plasma proteins such as albumin is lost in the urine (proteinuria), this results in reduced oncotic pressure, increased capillary filtration and excess fluid build-up (peripheral oedema) in the tissues which delays venous wound healing16. Deficiency of proteins impairs fibroblast proliferation and collagen synthesis during the proliferative phase16. Protein requirements are around 1-1.5g/kg body weight for wounds without exudates and up to 2g/kg body weight for wounds with exudate22. More than 2g/kg of body weight is known to increase oncotic pressure16 affecting hydration and delaying wound healing22. Meal plans should contain 20-25% protein22 from animals sources (meat, fish, chicken, eggs, dairy, etc.), and/or vegetarian sources (legumes, nuts, soy products28, etc.), whey or plant based protein powders and protein isolates35. In some studies, certain amino acids, such as Arginine and Glutamine, have been shown to enhance wound healing16, 18, 24, 28, 33, leading to some wound specific oral nutrition supplements containing these nutrients18, 22, 24, 33, 35.
People with impaired renal function like acute kidney injury (AKI), chronic kidney disease (CKD) and end stage renal disease (ESRD) are pre-disposed to several types of wounds38. The risk factors for poor wound healing in this group among others include suboptimally managed diabetes, ageing, trauma, burns, vasculitis, pharmacotoxicity, chronic venous insufficiency, neuropathy and peripheral arterial/vascular disease. In ESRD, uraemia, uraemic pruritus and calciphylaxis impair wound healing. Researchers report that people on haemodialysis lose 6-8g of protein/procedure while those on peritoneal dialysis lose 8-20g/day from the peritoneal cavity38 adversely affecting wound healing. Hence nutrition supplementation is important and needs to be monitored carefully. Proteins along with fat-soluble vitamins (A, D, E, K), water-soluble vitamins (B, C) and minerals (potassium, phosphorous, zinc, selenium, iron) are altered during the process of dialysis and need to be replenished/maintained at adequate levels for optimal wound healing38. In CKD stage 1 and 2 proteins are not usually restricted for wound healing and is the same as in healthy individuals with chronic wounds39. While in CKD stage 3 and 4 recommendations vary from 0.6-0.75g/kg of body weight to limit urea accumulation in the body39.
Fats provide signalling molecules and energy thus sparing proteins for wound healing and structural functions during tissue growth16, 22, 26-28. They assist with absorption of fat-soluble vitamins, which produce important precursors in the inflammatory phase16. Higher intakes of monounsaturated fats and omega-6 fatty acids are thought to promote wound healing due to the presence of essential fatty acids22. While omega-3 supplementation in some studies has been shown to decrease wound tensile strength16, 33, it has also been shown to decrease pressure ulcer progression, when combined with omega-6 fatty acids16, 37. Total intake of fat per meal should be 25-30% of total energy, with the majority of fats coming from polyunsaturated and monounsaturated sources. Deep sea fish, avocado, nuts and oilseeds are excellent sources of these fats35.
Vitamins and minerals have a range of functions including maintaining epithelial mucosal cells, stimulating collagen synthesis, facilitating immune function and improving wound healing and oxygenation. Micronutrient deficiencies delay wound healing16, 18, 22, 25-28, 33-35. In people with renal impairment the renal mechanisms to prevent hypervitaminosis is affected, therefore it is necessary to use caution during supplementation38.
Vitamin A stimulates epithelial growth, fibroblasts, and ground substance, increases monocytes and macrophages in the inflammatory phase, facilitates epithelial cell differentiation and has an anti-inflammatory effect on open wounds16, 33. Deficiency of vitamin A alters B and T-cell function and, antibody production in the inflammatory phase, while also impairing collagen synthesis in the remodelling phase16, 18, 28.
B-group vitamins act as coenzymes in the production of energy from macronutrients, maintain and support metabolic rate, maintain healthy muscle and skin tone, support immune and nerve function28, 34, 35. Folate and vitamin B6 are required in the production of red blood cells, while riboflavin and thiamine are needed for collagen formation and cross-linking18, 28, 34, 35. Meat, fish, dairy, some grains, vegetables and brewer’s yeast are good sources of vitamin B34.
Vitamin C influences collagen formation, antioxidant function and immuno-modulation in wound healing16, 18, 28, 33, 34. Deficiency of this vitamin impairs the immune response in the inflammatory phase, reduces collagen tensile strength and synthesis, and increases capillary fragility in the proliferative and remodelling phases16, 18, 28. For wound healing there is a recommendation to provide 500-1000mg vitamin C daily in divided doses and up to 2g/day in severe wounds (burns)16.
Vitamin D is involved in inhibiting secretion of calcitonin and parathyroid hormones (which increases calcium uptake and metabolism). These hormones are involved in neuromuscular and immune function, bone and cartilage remodelling necessary for wound healing34. Vitamin D also induces an anti-microbial peptide cathelicidin which promotes wound healing16, and vitamin D’s receptor signalling modulates structural integrity in addition to epithelial barrier transport function in wound repair16, 28. Fatty fish, beef liver, eggs34 and certain mushrooms40contain vitamin D.
Vitamin E is an antioxidant needed for fat metabolism and collagenation18, 35. It also stabilises cellular membrane integrity28, 33.
Vitamin K is needed for coagulation and bone metabolism during the haemostasis phase of wound healing34. Meat, dairy, eggs, avocado, green leafy vegetables, parsley and kiwi fruit are rich sources34.
Minerals like zinc, selenium and iron may have a role in wound healing:18, 32, 33 as anti-oxidants and cell replication modulators, tissue repair and growth promotors and in nucleic acid metabolism16, 18, 28, 33. All phases of wound healing are affected by zinc deficiency: in the inflammatory phase, higher susceptibility to infections and lower immunity; in proliferative phase, impaired wound tensile strength and collagen formation; and in the remodelling phase, reduced fibroblast proliferation, epithelialisation and collagen production16. Current recommendation for zinc supplementation, if deficient, is 40-220mg/day in divided doses for two weeks16, 34. Excess supplementation interferes with iron and copper absorption16, 18. Selenium has some antioxidant function which is beneficial in wound healing16, 34. Iron as a co-factor in collagen synthesis is thought to have a beneficial effect in wound healing16, 18 but supplementation has not shown any benefit. In people with iron deficiency anaemia (known to impair wound healing) there is tissue hypoxia and supplementation increases oxygen transport to proliferating tissues16, 34.
In CKD, sodium, potassium and phosphorous may need to be limited as these affect the kidneys and also delay wound healing38, 39. Supplemental nutrients are only recommended if there is a clinically diagnosed deficiency. Both overfeeding and underfeeding micronutrients (by supplementation) can deter wound healing23, 38. It is, however, important to ensure that a nutrient dense diet including wholegrains, proteins, dairy, vegetables and fruits provide these essential vitamins and minerals.
Hydration is very important in wound healing28 as fluids maintain skin turgor32 and promote tissue perfusion and oxygenation16. Blood flow and nutrient supply to the wound is affected by poor hydration thus slowing the progress of wound healing. Both over-hydration and dehydration can affect wound healing negatively35. There are three types of hydration issues: hypotonic, hypertonic and isotonic35. Water acts as a carrier solvent to transport nutrients and other molecules in and out of cells35. Recommendations are 35ml/kg of body weight of water for adults and 30ml/kg of body weight for people over 55 years, with a minimum of 1.5-2L/day22. In certain clinical states such as cardiac or renal conditions, fever, diarrhoea32, vomiting and diuresis16 there are individual variations, while with extensive exudates, fluid requirements could be higher22, 32. Generally for hydration water is preferred to other fluids16 except in under/malnourished states.
In cases of chronic alcohol consumption or alcoholic cirrhosis, liver and serum have depleted zinc and selenium levels, and supplementation improves nutrient levels and wound healing16. Narcotic use (prescription/recreational) can result in glycaemic variations, inadequate oral intake, constipation, nausea and anorexia, leading to increased nutritional deficiencies and delayed wound healing16.
The impact of nutrition on wound healing highlights the need for nutrition assessment and intervention to be part of standard practice in all phases of wound care to support optimal wound healing16, 22, 25-28, 30, 32-35. A detailed nutrition assessment conducted by a dietitian16, 28, 35 will identify the needs of an individual requiring nutritional support for wound care (including requirements for normal function, tissue regeneration, tissue repair and replacement of nutrients lost in wound exudates)23, 26. Measurement of nutrient losses is based on wound size and exudate volume14. Regular monitoring of nutrition is also valuable to prevent a decline in nutrition status, which can delay wound healing, affect quality of life and increase costs for both the client and the health system26, 27.
Conclusion
Key Messages
- Wounds are complex with varied aetiology; they could be acute or chronic and require a multifaceted nutrition approach
- General health, adequate nutrition, balanced diet and hydration status all have a direct impact on wound healing
- Hydration status should be monitored to ensure optimal hydration
- A nutritious diet for people with wounds should include 40-50% of energy from carbohydrates (wholegrains, vegetables and fruits), 20-25% proteins (animal and/or plant sources) and 25-30% healthy fats (nuts, oilseeds and avocado)
- Intake of energy, macronutrients and micronutrients play a vital role in wound healing
- Age, lifestyle, medications, comorbidities, physical, economic and psycho-social status influence wound healing and thus should be considered by those caring for people with wounds
- Overweight and obesity is associated with slower wound healing. However, planning weight loss during wound healing is counterproductive
- Wound assessments should routinely include the assessment of nutrition status using a validated nutrition screening tool such as the Malnutrition Screening Tool41 or Mini Nutritional Assessment40
- Treating malnutrition before addressing micronutrient deficiencies improves wound healing outcomes
- People with chronic wounds should be referred to a dietitian for specialised nutrition support
Acknowledgements
Dr. Madeleine Nowak PhD, APD, AN
James Cook University
References
1.Ousey K, Chadwick P, JawieÅ A, Tariq G, Nair HKR, Lázaro-MartÃnez JL, et al. Identifying and treating foot ulcers in patients with diabetes: saving feet, legs and lives. Journal of Wound             Care. 2018;27(Sup5):S1-S52. PubMed PMID: 29738280.
2.Han G, Ceilley R. Chronic Wound Healing: A Review of Current Management and Treatments. Advances in therapy. 2017;34(3):599-610. PubMed PMID: 28108895. Epub 2017/01/21. eng.
3.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004 May;27(5):1047-53. PubMed PMID: Â Â Â Â Â Â Â Â Â Â Â Â 15111519. Epub 2004/04/28. Yes.
4.Wound Management Innovation CRC. Wound CRC : Healing Wounds [webpage]. http://www.woundcrc.com/; 2013 [updated 2013 Wound Management Innovation CRC; Â Â cited 2014 6/05/2014].
5.Whitlock E, Morcom J, Spurling G, Janamian T, Ryan S. Wound care costs in general practice             A cross-sectional study. Australian Family Physician. 2014 3/01;43:143-6.
6.Agale SV. Chronic Leg Ulcers: Epidemiology, Aetiopathogenesis, and Management. Ulcers. 2013;2013:9.
7.Wild TMD, Rahbarnia A, Kellner M, Sobotka LMDPD, Eberlein TMD. Basics in nutrition and wound healing. Nutrition. 2010;26(9):862-6.
8.Society WH. Wound Care Guidelines. 2006.
9.Reddy M, Cottrill R, Cansino V. Healing Wounds, Healthy Skin A Practical Guide for Patients with Chronic Wounds: Yale University Press; 2011.
10.Bhattacharya S, Mishra RK. Pressure ulcers: Current understanding and newer modalities of      treatment. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2015;48(1):4-16.
11.Youn YJ, Lee J. Chronic venous insufficiency and varicose veins of the lower extremities. The Korean journal of internal medicine. 2019;34(2):269-83.
12.Michael JE, Maier M. Lower extremity ulcers. Vasc Med. 2016 Apr;21(2):174-6. PubMed PMID: 26858182. Epub 2016/02/10.
13.Hedayati N, Carson JG, Chi Y-W, Link D. Management of mixed arterial venous lower extremity ulceration: A review. Vascular Medicine. 2015;20(5):479-86. PubMed PMID: Â Â Â Â Â Â Â 26206851.
14.Barber GA, Weller CD, Gibson SJ. Effects and associations of nutrition in patients with venous leg ulcers: A systematic review. J Adv Nurs. 2018 Apr;74(4):774-87. PubMed PMID: Â Â Â Â Â Â Â Â Â Â 28985441. Epub 2017/10/07.
15.Fukaya E, Margolis DJ. Approach to diagnosing lower extremity ulcers. Dermatologic Therapy. 2013;26(3):181-6.
16.Quain AM, Khardori NM. Nutrition in Wound Care Management: A Comprehensive              Overview. Wounds. 2015;27(12):327-35.
17.MacLellan D. Chronic Wound Mangement. Australian Prescriber. 2000;23(1):6-9.
18.Longmore B. The complementary approach: The role of nutrition in wound healing. Australian Pharmacist. 2015;34(3):54-7.
19.Werdin F, Tennenhaus M, Schaller H-E, Rennekampff H-O. Evidence-based management strategies for treatment of chronic wounds. Eplasty. 2009;9:e19-e. PubMed PMID: 19578487.
20.Rizvi AA. Nutritional challenges in the elderly with diabetes. International Journal of Diabetes Mellitus. 2009;1(1):26-31.
21.ADA. Standards of Medical Care in Diabetes. Diabetes Care. 2004;28(Supplement 1):S4-S36.
22.Dawson B. Wound Healing, Nutrition and Aging. Geriatric medicine in general practice. 2011 04/2011;8(2011):10-1.
23.Skipper A. Challenges in Nutrition, Pressure Ulcers, and Wound Healing. Nutrition in Clinical        Practice. 2010;25(1):13-5.
24.Mulholland GD. Supplements to promote wound healing. MedSurg Nursing. 2015 2015 January-February:S2+.
25.Barratt N. Nutrition and Wound Healing: Implications for Practice. Journal of the Dermatology Nursesâ Association. 2014;6(1):27-32.
26.Bishop A, Witts S, Martin T. Role of nutrtiion in successful wound healing. Jourmal of Community Nursing. 2018;32(4):44, 6, 8-50.
27.Molnar JA, Underdown MJ, Clark WA. Nutrition and Chronic Wounds. Advances in wound care. 2014;3(11):663-81. PubMed PMID: 25371850. eng.
28.Dryden SV, Shoemaker WG, Kim JH. Wound Management and Nutrition for Optimal Wound Healing. Atlas of the Oral & Maxillofacial Surgery Clinics of North A. 2013;21(1):37-47.
29.Morgan Y. Surgical Wound Healing. The Dissector: Journal of the Perioperative Nurses College of the New Zealand Nurses Organisation. 2019 2019/06////;47:34+. English.
30.Fuhrman MP. Wound Healing and Nutrition. Topics in Clinical Nutrition. 2003;18(2):100-10.
31.Abreu AM, Oliveira DWD, Marinho SA, Lima NL, de Miranda JL, Verli FD. Effect of Topical Application of Different Substances on Fibroplasia in Cutaneous Surgical Wounds. ISRN Â Â Â Â Â Dermatology. 2012;2012:5.
32.Taylor C. Nutrition and pressure ulcers putting evidence into practice. Journal of Community Nursing. 2016;30(4):38, 40, 2, 4.
33.Kavalukas SL, Barbul A. Nutrition and wound healing: an update. Plastic and reconstructive surgery. 2011;127 Suppl 1:38S-43S.
34.Brown KL, Phillips TJ. Nutrition and wound healing. Clinics in Dermatology. 2010 2010/07/01/;28(4):432-9.
35.Posthauer ME. Nutrition: a critical component of wound healing. Advances in skin & wound care. 2010 12/2010;23(12):560-72.
36.Bemak L. Nutrition and Wound Healing. AJN The American Journal of Nursing. 2018;118(6):13. PubMed PMID: 00000446-201806000-00003.
37.Bolton L. The Power of Nutrition. Wounds. 2010;22(12).
38.Maroz N, Simman R. Wound Healing in Patients With Impaired Kidney Function. The journal    of the American College of Clinical Wound Specialists. 2014;5(1):2-7. PubMed PMID:           26199882. eng.
39.Collins N. Nutrition 411: nutrition for the patient with chronic kidney disease and wounds. Ostomy Wound Management. 2011;57(9):16-9. PubMed PMID: 108198772. Language: English. Entry Date: 20120106. Revision Date: 20150819. Publication Type: Journal Article. Journal Subset: Core Nursing.
40.Cardwell G, Bornman JF, James AP, Black LJ. A Review of Mushrooms as a Potential Source of Dietary Vitamin D. Nutrients. 2018;10(10):1498. PubMed PMID: 30322118. eng.
41.Ferguson M, Capra S, Bauer J, Banks M. Development of a valid and reliable malnutrition screening tool for adult acute hospital patients. Nutrition. 1999;15(6):458-64.