The Perceptions and Impact of a Health Professional Mentoring Program for Multidisciplinary Diabetes Educators in Australia: A Quantitative Study

Introduction
Aims: The purpose of the project was to explore the perceptions of participants who completed the Australian Diabetes Educators Association (ADEA) mentoring program.
Methods: The study used a quantitative exploratory study methodology. An online survey through SurveyMonkey, was utilised which included demographic data, a variety of question types and 25 Likert scale statements to explore the perceptions and impact of the mentoring program.
Results: A total of 75 diabetes educators who had participated in the ADEA mentoring program, either as a mentor or mentee, completed the survey, with 69% (n = 52) being mentors and 31% (n = 23) mentees, 97% females and 96% Registered Nurses. A total of 56% (n = 40) of participants perceived the most important benefit of cross-disciplinary mentoring to be interdisciplinary collaboration, followed by 25% (n = 18) perceiving a greater understanding of differing scopes of practice. Of the 25 Likert scale statements, three statements yielded statistically significant responses between mentors and mentees, regarding the usefulness of online resources, the program mentoring manual and organisational support to undertake mentoring.
Conclusion: The ADEA mentoring program resources were deemed to require review and refinement, clearer guidelines for goal setting, clarity of roles, and clearly defined responsibilities within the mentoring partnership. Further research is needed to assess differing requirements of cross-disciplinary mentoring. The study provided recommendations for further research of mentoring programs, including the provision of feedback within mentoring, the format of mentoring programs and logistics, formation of mentoring partnerships, and organisational support required to undertake mentoring.
Key Words: Diabetes, Education, Mentorship
Funding
This project received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. The authors declare there is no conflict of interest.
Introduction
The purpose of the study was to explore the perceptions of a health professional mentoring program for diabetes educators in an Australian context. The project aimed to add strength and knowledge of the perceptions and impact of the current ADEA mentoring program in order to further improve its design and use in the future. A broader aim of the project was to add to the body of knowledge for the development and use of cross-disciplinary health professional mentoring programs. The focus themes identified for exploration included the benefits of mentoring, barriers to effective mentoring and strategies/enablers to effective mentoring.
The benefits of mentoring have been well documented in the literature and include development and refreshment of professional skills and knowledge, networking with colleagues, feeling professionally connected, the development of confidence and leadership, and feeling empowered and satisfied from participating2-5. Barriers include the time required to commit to a mentoring partnership, lack of organisational support, miscommunication, and mismatches between mentors and mentees2, 6. Many studies have also detailed strategies to ensure the effectiveness of mentoring programs. The expectations, objectives, roles and responsibilities and timeline of a mentoring partnership should be realistic, with the commitment agreed upon by mentors and mentees2, 3. A successful mentoring partnership relies on building a mutual connection based on trust, respect, flexibility and commitment and was also described as more effective if mentors and mentees mutually select each other2, 6, 7, 8. The use of training and resources also enhanced the effectiveness of mentoring and varies between mentors and mentees, with formal, structured programs shown to be most effective, due to the clear and documented expectations of roles and objectives2, 3, 5, 6, 9. Overall, mentoring has been used across a wide variety of professions, for the intention of personal and professional development, through a relationship based on support, guidance and feedback4.
Methods
Study design
A quantitative exploratory study design was utilised to investigate the experience of the ADEA mentoring program for diabetes educators. A survey was developed by the authors to explore the perceptions and impact of the mentoring program. A literature search revealed no existing appropriate tools to measure perceptions and impact of mentoring programs or specific for use. The survey included demographic data, closed-ended questions, multiple-choice questions, and 25 statements, utilising a 5-point Likert scale. The survey was reviewed for content and face validity by five academics and five diabetes education experts. The five diabetes education experts consisted of a novice mentee, an experienced mentor, two diabetes education academics, and the Manager of Professional Services and Education from the ADEA National Office. A Content Validity Index (CVI) process was used to ensure each item / statement to be measured was relevant and clear to the topic, and the survey was amended following recommendations from the experts resulting in changes in language and the removal of suggestive wording such as leading questions. The survey was reviewed ten times with a final version entered into the online software SurveyMonkey. The survey recorded demographic data, followed by closed-ended questions, yes/no/unsure questions, and tick box responses to questions. A total of 25 positive and negative statements, utilising a 5-point Likert scale were used to measure participant responses aiming to reveal attitudes and viewpoints towards each statement.
Population and recruitment
The sample population consisted of members of the ADEA, who were currently either a mentor or mentee. In 2019, there were 2348 ADEA members across Australia, from various primary health professions, and 95 mentoring partnerships registered10. Participants were recruited nationally using convenience sampling via an email invitation sent to ADEA members. The email included an introduction of the research, benefits of the research, a plain language information statement and a link to the survey. The survey was open for a period of five weeks, with implied consent assumed on completion of the survey.
Ethical considerations
Approval to undertake the research was gained from the Federation University Australia Human Research Ethics Committee following a standard application (Approval no. A19-085). External approval was also gained from the Chief Executive Officer of the ADEA.
Data analysis
The quantitative data set collected was analysed using descriptive and inferential statistics. The survey responses collected via SurveyMonkey were exported into an Excel file and imported into SPSS, version 251. Data was cleaned to remove outliers and missing data from participants who failed to answer questions or respond to items in the survey. Descriptive analysis was used to summarise the demographic data of the participants, including number of mentors/mentees, age, gender, primary profession, length of time involved in the ADEA mentoring program, and number of times a participant had undertaken the role of a mentor. Independent t-tests were used to test for significant differences in responses to statements between the two independent samples, mentors and mentees11. The t-testing enabled the researchers to compare the results from independent samples, utilising the mean scores on a continuous variable12. Therefore, the independent sample t-test determined whether there was a statistically significant difference in mean scores of mentors and mentees12. Utilising the Levene’s test for equality of variances of the two groups (mentors/ mentees), equal variances were not assumed as the p < 0.05. A statistically significant difference in mean scores of mentors and mentees was reported if the significance (2-tailed) was equal or less than 0.0512.
Results
Of the 75 participants, 69% (n = 52) were mentors, while 31% (n = 23) were mentees, ranging in age from 20s to 69 (see Figure 1) of which 3% (n = 2) were male and 97% (n = 73) were female. The primary profession of the participants included 96% (n = 71) Registered Nurses, with the remaining 4% being an Accredited Practising Dietitian (n = 1), a Pharmacist (n = 1) and a Registered Midwife (n = 1). Most participants were from Victoria, with all states represented except for the Northern Territory and Australian Capital Territory (see Figure 2).
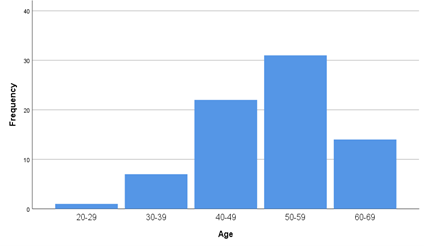 Figure 1: Age of Participants
Figure 1: Age of Participants
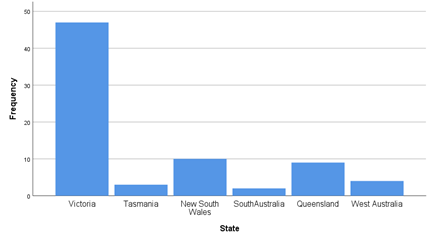 Figure 2: State of participants
Figure 2: State of participants
The length of time participants were involved in the ADEA mentoring program ranged from 6 months or less, to 11 or more years (see Figure 3). For mentors, the number of times they had mentored a diabetes educator for initial credentialling ranged from one to three times, to more than 16 times. Approximately half of the mentors, 49% (n = 25), were listed as an available mentor on the ADEA website. Many of the participants who were not listed reported that this was because they did not feel they had enough experience to mentor others.
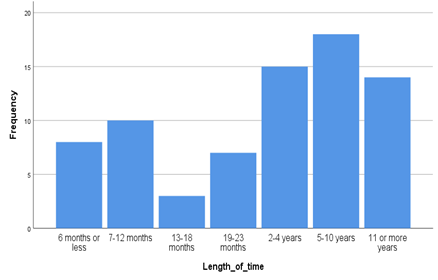
Figure 3: Length of time participants involved in ADEA mentoring program
When asked about the perceived benefits of cross-disciplinary mentoring, participants reported the biggest benefits to be interdisciplinary collaboration (56%), developing a greater understanding of scope of practice (25%), and the opportunity for broader networking (8%). A total of 11% (n = 8) perceived there were no benefits of interdisciplinary mentoring.
When asked if they would mentor, or be mentored by a diabetes educator outside their primary discipline in the future, 49% (n = 37) reported “yes”, 23% (n = 17) said “no” and 28% (n = 21) were unsure. For those that responded “yes”, there was a focus on a greater understanding of the role and scope of practice of the different disciplines, learning from each other, and promoting interdisciplinary cooperation. For those who responded “no”, their rationale included concerns about difficulty understanding each other’s specific roles and scope of practice. The means in which mentoring partnerships were established included 35% (n = 18) through a workplace colleague, 31% (n = 16) via the ADEA website, 17% (n = 9) were recommended by a friend or colleague, 11% (n = 6) due to a previous clinical placement, and 6% (n = 3) from attending a conference or other meeting.
There were only three statements that yielded statistically different responses between mentors and mentees from the 25 Likert scale statements (Table 1, highlighted in blue). Two statements related to the ADEA resources being utilised as part of the mentoring program, and one related to support from one’s workplace to undertake the mentoring program. There was a statistically significant difference between mentors and mentees with response to the statement “The ADEA online resources were useful” (t = 2.262, p = .032). Although both neither agreed nor disagreed, mentees perceived the resources were more beneficial than mentors. Responses to the statement “The ADEA mentoring manual did not meet my learning needs”, were also statistically significant between mentors and mentees (t = 3.738, p = .001). Mentors did not perceive the manual met their learning needs, while mentees neither agreed nor disagreed. With regard to mentoring logistics, mentors disagreed with the statement “I received adequate support from my workplace to undertake the mentoring program”, while mentees neither agreed nor disagreed (t = 2.530, p = .016). Mentors perceived their workplaces as not supportive when mentoring novice diabetes educators towards credentialling, while mentees were unsure. Of the remaining 22 statements (as per Tables 2 and 3), both mentor and mentee responses were similar regarding all aspects of mentoring and the program itself.
Table 1: Inferential Statistically Significant Responses to Likert Scale Statements
| Statement | Mentor (n=X/mean) | Mentee (n=X/mean) | t | Sig. 2-tailed | ||
| The ADEA online resources were useful. | 37 | 3.70 | 17 | 3.12 | 2.262 | .032 |
| The ADEA mentoring manual did not meet my learning needs. | 37 | 3.12 | 17 | 2.43 | 3.738 | .001 |
| I received adequate support from my workplace to undertake the mentoring program. | 51 | 2.73 | 23 | 3.39 | 2.530 | .016 |
Table 2: Inferential Statistical Results of Positive Likert Scale Statements
| Statement | Mentor (n=X/mean) | Mentee (n=X/mean) | t | Sig. 2-tailed | ||
| I enjoyed participating in the ADEA mentoring program. | 37 | 4.11 | 17 | 3.71 | 1.378 | .179 |
| It was easy to develop goals for the mentoring program. | 37 | 3.68 | 17 | 3.35 | 1.512 | .140 |
| Feedback is important to build confidence. | 52 | 4.31 | 23 | 4.61 | 1.856 | .068 |
| Feedback provided should always be constructive. | 52 | 4.13 | 23 | 4.43 | 1.651 | .103 |
| Enthusiasm is an important attribute for a mentor/ mentee. | 52 | 4.38 | 23 | 4.39 | 0.042 | .967 |
| I learnt things about myself through the mentoring program. | 52 | 4.00 | 23 | 3.83 | 0.938 | .353 |
| My role and responsibilities as a mentor/ mentee were clear to me. | 52 | 3.94 | 23 | 3.74 | 0.896 | .378 |
| This program helps me to reflect on my scope of practice. | 52 | 4.12 | 23 | 3.87 | 1.283 | .206 |
| Participating in the mentoring program has positively changed my professional practice. | 52 | 4.12 | 23 | 3.74 | 0.122 | .903 |
| Self-reflection is an important skill to develop and maintain. | 52 | 4.46 | 23 | 4.57 | 0.723 | .473 |
| Technology helped me connect easier with my mentor/ mentee. | 51 | 3.94 | 23 | 3.96 | 0.089 | .929 |
| Face-to-face meetings were the most beneficial. | 51 | 3.75 | 23 | 3.74 | 0.026 | .980 |
| The mentoring partnership was of adequate length. | 51 | 4.00 | 23 | 3.78 | 1.443 | .156 |
| The mentoring program is valuable to my profession. | 50 | 4.24 | 22 | 4.05 | 0.951 | .348 |
| The mentoring program helps establish supportive relationships. | 50 | 4.34 | 22 | 4.05 | 1.680 | .102 |
| The mentoring program is an opportunity for personal and professional growth. | 50 | 4.42 | 22 | 4.00 | 1.865 | .073 |
Table 3: Inferential Statistical Results of Negative Likert Scale Statements
| Statement | Mentor (n=X/mean) | Mentee (n=X/mean) | t | Sig. 2-tailed | ||
| The ADEA mentoring program did not meet my expectations. | 37 | 2.41 | 17 | 2.88 | 1.740 | 0.94 |
| My mentor/ mentee was difficult to engage with. | 52 | 1.96 | 23 | 1.70 | 1.086 | .283 |
| My mentor/ mentee had unrealistic expectations. | 52 | 2.10 | 23 | 1.83 | 1.392 | .170 |
| It was difficult to devote appropriate time to the program. | 51 | 2.94 | 23 | 2.83 | 0.468 | .642 |
| The mentoring program is a waste of time. | 50 | 1.60 | 22 | 1.95 | 1.843 | .074 |
| The mentoring program is not important for a diabetes educator to become credentialled. | 50 | 1.78 | 22 | 2.27 | 1.816 | .078 |
Discussion
Barriers to effective mentoring include, the time to commit to mentoring, lack of organisational support, miscommunication, and inappropriate matching of mentors and mentees2, 5, 6. Unlike previous studies which have reported time constraints as a barrier to participation in a mentoring program, participants in the current study believed it was easy to devote appropriate time to the program (see Table 3). At present the ADEA mentoring program is set to a minimum of six months, however each partnership is self-directed and the partnership may last for as long as each member deems appropriate. Participants in the current study neither agreed nor disagreed that technology helped them connect with their mentoring partner, or that face-to-face meetings was the most beneficial form of communication, which could lend itself to trialling online versions of mentoring in the future[8]. In the current study, there was a statistically significant difference between mentors and mentees with respect to organisational support, with mentors perceiving that they did not receive support and mentees being unsure.
A lack of communication and mismatch between mentors and mentees have been identified as barriers to effective mentoring2. In the current study both mentors and mentees perceived their mentor or mentee to be easy to engage with. These findings could indicate that the self-selection of mentors and mentees in the ADEA mentoring program was a positive quality of the program, and supports the findings of a previous study regarding mentoring success with mutual selection of partnerships6.
Effective mentoring strategies include developing clear partnership objectives, defining roles and responsibilities of mentors and mentees, and the inclusion of resources and training to support participants,2-4, 8. Previous studies suggest the expectations, roles, responsibilities, and objectives of a mentoring partnership should be realistic and agreed upon by both mentors and mentees at the beginning of the partnership2, 3. In the current study, both mentors and mentees were unsure of their roles and responsibilities for developing goals for participation in the ADEA mentoring program. These results are interesting, as the same participants also perceived the mentoring program met their expectations and perceived their partner’s expectations to be realistic. These results may indicate the overall strength and positive use of the program, despite participants not being clear on their roles. Previous studies also focused on the training and resources to enhance the effectiveness of mentoring programs2, 3, 5, 9. In the current study there was a statistically significant difference in the perceptions of mentors and mentees regarding the ADEA online resources. Mentors in the current study agreed that the ADEA mentoring manual met their learning needs, while mentees neither agreed nor disagreed. This could indicate the need for further development of current ADEA mentoring program resources.
Both mentor and mentee participants in the study agreed that feedback was important to build confidence and should always be constructive, suggesting that the use of formal feedback could be an enabler to promote effective mentoring. Previous research has identified] the ability to give feedback as an essential skill to develop in the course of becoming a valuable mentor6. In the current study, a significant proportion of the participants had been involved in the ADEA mentoring program for five to ten years (24%), or more than 11 years (19%), which could suggest the experience of participants was a factor when providing constructive feedback. These results may also indicate the need for information and resources on how to give constructive feedback, especially for new mentors.
Limitations
There were recognised limitations of the current study. Missing data resulted in 23 participants being excluded from the study due to incomplete question responses which significantly reduced the sample size. Another potential limitation of the survey tool was the positive skew of the statements. While the researchers aimed to include both positive and negative statements to avoid bias, the skewed positive outlook of the survey may have altered participant interpretation of the survey. Consideration should be given whether the inclusion of matching pairs of mentors and mentees, in particular mentoring partnerships, may have yielded different findings of the study13. Given that over two thirds of the total number of participants were mentors, this may have impacted the validity of the study11. The study also did not ask participants about whether they had taken part in an interdisciplinary mentoring relationship, only their perception of the same, which could have produced different results. In addition, the generalisability of the current study may also be impacted due to the low percentages of participants from varying disciplines.
Implications/ Recommendations
The current study highlights recommendations for the future of the ADEA mentoring program, and mentoring on a broader level. Specific to the ADEA mentoring program, existing resources should be reviewed and refined, enabling clearer guidelines for goal setting, providing and receiving constructive feedback, and role, and responsibilities within the mentoring partnership. Further research is also proposed to assess the various requirements of cross-disciplinary mentoring and the provision of constructive feedback. Due to the evolving nature of the role and scope of diabetes educators’ practice across varying health professional backgrounds, the findings of this study into the ADEA mentoring program warrants ongoing revision to ensure the needs of all health professionals are being met.
Conclusion
The findings of this study provide a valuable insight into the mentoring relationships of diabetes educators. Further research on mentoring programs should investigate the provision of feedback within mentoring, formation of mentoring partnerships, and organisational support required to undertake mentoring. The insightful perceptions of diabetes educators who have participated in the ADEA mentoring program could assist in the enhancement of future mentoring programs across many disciplines. The study also adds value to the ongoing professional development of diabetes educators, which in turn positively impacts the care provided to people with diabetes.
Acknowledgements
The authors wish to thank the Australian Diabetes Educators Association (ADEA) for their support to undertake this study.
References
1.IBM Corp, IBM SPSS Statistics for Windows, Version 25. 2017, IBM Corp: Armonk, NY.
2.Browne, J., et al., A qualitative evaluation of a mentoring program for Aboriginal health workers and allied health professionals. Australian and New Zealand Journal of Public Health, 2013. 37(5): p. 457-462.
3.Beck, J.K. and S.E. Traficano, Diabetes Educator Mentorship Program. The Diabetes Educator, 2015. 41(1): p. 38-42.
4.Harris, S., Development of the perceptions of mentoring relationships survey: A mixed methods approach. International Journal of Multiple Research Approaches, 2013. 7(1): p. 83-95.
5.Modic, M.B., et al., A Diabetes Management Mentor Program. Clinical Nurse Specialist, 2012. September/October: p. 263-271.
6.Huybrecht, S., et al., Mentoring in nursing education: Perceived characteristics of mentors and the consequences of mentorship. Nurse Education Today, 2011. 31: p. 274-278.
7.O’Connell, E.O., M. Stoneham, and J. Saunders, Planning for the next generation of public health advocates: evaluation of an online advocacy mentoring program. Health Promotion Journal of Australia, 2016. 27: p. 43-47.
8.Wilson, A.H., S. Sanner, and L.E. McAllister, An Evaluation Study of a mentoring program to increase the diversity of the nursing workforce. Journal of cultural diversity, 2010. 17(4): p. 144-150.
9.Ndayisaba, A., et al., A clinical mentorship and quality improvement program to support health center nurses manage type 2 diabetes in rural Rwanda. Journal of Diabetes Research, 2017: p. 1-10.
10.Australian Diabetes Educators Association, Member database. 2020: Woden.
11.Burns, N. and S.K. Grove, The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence. 2009, St Louis: Saunders Elsevier.
12.Pallant, J., SPSS Survival Manual. 3rd ed. 2007, Crows Nest: Allen & Unwin
13.Polit, D., F and C.T. Beck, Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. 2012, Philadelphia: Lippincott Williams & Wilkins.