Alcohol and Type 2 Diabetes: Do They Mix?
Introduction
Alcohol is the most commonly used recreational drug in Australia and is consumed to varying degrees in a multitude of social and cultural settings. It is estimated that one-in-six people consume alcohol at levels that place them at lifetime risk of an alcohol-related disease or injury.1 The short-term and long-term consequences of alcohol use on physical, psychological and social well-being have been extensively researched and well-documented. However, in people with diabetes, the effects of alcohol may be amplified. Thus, it is imperative for clinicians and people with diabetes to understand the effect of alcohol on the progression and complications of the condition.
Diabetes affects over one in twenty Australians (1.2 million people) and has multi-system complications including cardiovascular disease, kidney disease, stroke, limb amputation, blindness and anxiety/depression, that can severely impact an individual’s quality of life.2, 3 The total cost for Australians living with diabetes is in excess of $20 billion annually and poses a significant financial burden to individuals and the healthcare system.4
This article seeks to summarise the current state of knowledge regarding the pathophysiological mechanism of alcohol’s effects on glycaemic management; the impact of alcohol consumption on the management of diabetes and practical tips for managing alcohol use in people with diabetes.
Pathophysiological mechanisms between alcohol and diabetes
Diabetes is a chronic condition characterised by the body’s inability to produce insulin (type 1 diabetes, T1D) or an inability to respond to circulating insulin (type 2 diabetes, T2D). Insulin is a hormone produced by the pancreas and is responsible for regulating blood glucose levels (BGLs).5
Numerous studies have investigated the mechanisms that underlie the effect of alcohol consumption on glycaemic control in people with diabetes. These effects differ substantially depending on whether alcohol consumption occurs during the ‘fed state’ (when the person has just eaten and BGLs are high) or in the ‘fasting state’ (when the person has not eaten for several hours or days and BGLs are low).
The fed state
In the fed state (i.e. 4 hours post-eating), acute episodes of alcohol consumption do not lead to clinically significant changes in BGLs.6 Conversely, chronic alcohol use in well-nourished individuals with diabetes can result in long-term hyperglycaemia.7 This makes people with diabetes with long-term excessive use of alcohol more susceptible to the micro- and macrovascular complications of the condition.
The fasting state
In the fasting state (i.e. greater than 8 hours post-eating), alcohol consumption can result in profound hypoglycaemia which can have fatal consequences (coma or death) as there is insufficient glucose to maintain brain function.8 This is seen when alcohol is consumed for days without adequate dietary intake.
In the fasting state, the body has two major mechanisms for maintaining BGLs – 1) glycogenolysis or the breakdown of glycogen stored in the liver to produce glucose and 2) gluconeogenesis which is the synthesis and release of new glucose by the liver. Insufficient dietary intake can stop glycogenolysis after 1-2 days and the liver prioritises alcohol metabolism over gluconeogenesis, resulting in decreased glucose production and hypoglycaemia.
Alcohol consumption can also lead to hypoglycaemic unawareness where an individual is unable to recognise the symptoms of hypoglycaemia.9 In addition, alcohol often delays a return to normal BGLs.10
The combination of alcohol-induced hypoglycaemia, hypoglycaemic unawareness and delayed recovery from hypoglycaemia can lead to incontinence, inability to follow simple commands, disorientation and reduced cognitive function. In some cases, these changes may not be reversible.11
Impact of alcohol on diabetes management
In people without diabetes, numerous studies have demonstrated that low to moderate levels of alcohol consumption can be protective against developing T2D.12-13 However, in people with known diabetes, alcohol amplifies the complications of the condition.
Weight gain
A key component of diabetes management is lifestyle modification and maintaining a healthy body weight. Alcohol has very little nutritional value and is high in energy. As a result, consumption of alcohol in large amounts or on a regular basis can lead to weight gain, which can make achieving optimal glycaemic management challenging.14 Obesity is also an independent risk factor for developing other major co-morbidities such as cardiovascular disease.15
Hyper/hypoglycaemia
Chronic heavy alcohol use impairs insulin secretion and reduces insulin sensitivity, leading to impaired glucose tolerance.16 Furthermore, consuming alcohol around mealtimes not only increases the energy density of the meal but also stimulates appetite and food intake which can lead to hyperglycaemia.14 Alcohol-induced hypoglycaemia has been observed in people with and without diabetes, but is significantly more dangerous in the former group due to already impaired insulin regulation.
Disease progression including complications
Long-term alcohol consumption has been associated with a greater incidence of short and long-term complications from diabetes.
Alcoholic ketoacidosis In people with diabetes, heavy alcohol consumption can precipitate alcoholic ketoacidosis (AKA), a condition characterised by extremely low insulin levels and excessive glucagon levels, resulting in the presence of ketone bodies in the blood. In AKA glucose levels are usually low to normal, compared to diabetic ketoacidosis (DKA) where they are usually significantly elevated.17 The metabolic acidosis can be made worse by repeated vomiting and dehydration. People suffering from AKA are usually lucid and alert despite the acidosis and marked ketonaemia, as compared to persons with DKA.18 Thus, clinicians treating people with diabetes with known heavy alcohol consumption should always be aware of the possibility of alcoholic ketoacidosis.
Lipid abnormalities Alcohol consumption is known to exacerbate diabetes-related lipid abnormalities, including elevated triglyceride levels and reduced low-density lipoprotein (LDL) cholesterol.19 Elevated triglyceride levels are an independent risk factor for cardiovascular disease.20 In addition, they can also cause pancreatitis that interferes with insulin production, thereby worsening glycaemic management.21 Furthermore, despite alcohol consumption lowering LDL-cholesterol, evidence suggests that the remaining LDL molecules exhibit altered biological functions (such as low vitamin E levels), which may have harmful long-term effects.22
Cardiovascular disease Evidence suggests that low to moderate alcohol consumption is associated with decreased cardiovascular mortality.23 However, alcohol consumption in excess of this is a known risk factor for both cardiovascular and cerebrovascular disease.
Liver disease Sustained heavy alcohol consumption or high frequency of alcohol consumption influences the risk of liver disease such as fatty liver, alcoholic hepatitis and alcoholic cirrhosis.24 Numerous studies indicate that people with non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) should abstain from alcohol consumption as there may be an increased risk of developing cancers.25-26
Peripheral neuropathy Diabetes and alcohol are the two major causes of peripheral neuropathy and numerous studies indicate that heavy alcohol consumption can increase the progression of neuropathy.27-28 Peripheral neuropathy is caused by a combination of narrowed small blood vessels and deposition of advanced glycated end-products, resulting in reduced sensory and motor functions of nerves. Sensory peripheral neuropathy makes it difficult for people with diabetes to sense pain or the presence of a wound on their lower limb, predisposing them to ulceration, infection and lower limb amputation.
Retinopathy Alcohol is believed to exacerbate diabetic retinopathy by causing oxidative stress on the retinal tissue.29 The United Kingdom Prospective Diabetes study confirmed that alcohol consumption in men with diabetes was associated with more severe retinopathy compared to those who didn’t drink alcohol.30
Erectile dysfunction In men, erectile dysfunction is a known complication of diabetes that can be exacerbated by chronic alcohol use.31 While the mechanisms underlying this association require further investigation, it is suggested that lower than normal levels of the sex hormone testosterone are implicated.32 Alcohol is known to further lower testosterone levels.33
Medication interactions
Alcohol interacts with numerous medications used to manage diabetes including:
Insulin: Heavy alcohol consumption in people who use insulin to manage their diabetes is associated with higher rates of severe hypoglycaemia and diabetic ketoacidosis.34
Sulfonylureas: Gliclazide (Diamicron), glibenclamide (Daonil) and chlorpropamide (Diabinese) have been known to induce long-periods of hypoglycaemia when taken in conjunction with alcohol. They also decrease the rate of ethanol elimination from the blood, resulting in a greater risk of alcohol toxicity.35
Chlorpropamide, glibenclamide, tolbutamide: Induce nausea and vomiting after alcohol consumption.35
Metformin: Excess alcohol consumption in conjunction with metformin increase the risk of developing lactic acidosis.35
Sodium glucose cotransporter 2 (SGLT2) inhibitors -dapagliflozin, empagliflozin, canagliflozin: excessive alcohol consumption in association with use of SGLT2 inhibitors may precipitate DKA in subjects with type 2 diabetes36.
Warfarin: Used for anticoagulation in people with known thrombosis or arrythmias who may have diabetes. Acute alcohol intake may increase anticoagulation by decreasing warfarin metabolism. Chronic alcohol ingestion may decrease anticoagulation by increasing warfarin metabolism.35
It is advisable that people with diabetes consult their doctor prior to consuming alcohol with medications in order to avoid any possible interactions.
Self-care behaviours
A significant factor in effective diabetes management is an individual’s capacity and willingness to carry out self-management strategies such as exercising, smoking cessation, blood glucose monitoring, taking diabetes medications, following a healthy diet and being linked in with a supportive multidisciplinary diabetes team. Evidence indicates that there is an inverse relationship between excessive alcohol consumption and effective diabetes self-management.37 This relationship is thought to have a multi-factorial aetiology as alcohol consumption is associated with:
- A reduced likelihood to follow dietary, exercise and medication recommendation12, 38-39
- Poor attendance at follow-up appointments with specialists and allied health services37
- Decrease frequency of glucose self-monitoring, leading to higher incidence of hypo and hyperglycaemic events40
All of the above can lead to suboptimal glycaemic management and increase the risk of complications and disease progression.
Practical tips for risk management
It is imperative for clinicians to understand the risks involved with alcohol consumption in people with diabetes. Furthermore, they must be able to communicate these risks and counsel people with diabetes on risk-reduction strategies.
How much alcohol is safe to drink?
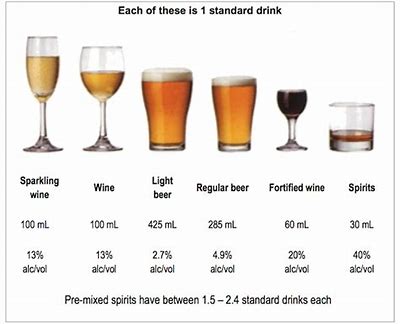
Current guidelines suggest no more than two standard drinks per day for both men and women.41 This is the same for people with and without diabetes. A standard drink contains 10g of alcohol. This is equivalent to:
- 285ml of mid- strength beer
- 30ml of spirits
- 100ml of wine

Figure 1: A standard drink36
It is important to educate people with diabetes regarding safe levels of alcohol consumption as this can reduce both the rate of disease progression and the risk of further complications. Certain population-groups such as women who are pregnant or planning a pregnancy and those under the age of 18 are advised to abstain from alcohol consumption altogether.41
What types of alcohol should people with diabetes choose?
Beverages high in sugars such as soft-drink mixers, sweet liqueurs and pre-mixed alcoholic beverages are more likely to increase BGLs. Instead, it is preferable to choose low-alcohol beers or spirits with diet mixers. Low-carbohydrate beers offer no advantage over regular beers as they often have a higher alcohol content which can worsen overall diabetes management.
Managing alcohol-induced hypoglycaemia42
Prevention is the best way to manage alcohol-induced hypoglycaemia. People with diabetes should be advised to drink alcohol responsibly and in moderation. This includes avoiding binge drinking and ingesting carbohydrates while consuming alcohol and before going to bed. People with diabetes should be educated that alcohol can reduce the awareness of hypoglycaemia and BGLs should be monitored more frequently (before bed and in the morning) to identify and reduce the risk of hypoglycaemia. In addition, it is advisable that people with diabetes wear some form of diabetes identification, otherwise other people may mistake symptoms of a hypoglycaemic episode as alcohol intoxication and fail to get help. It is also recommended that when consuming alcohol, people with diabetes have someone else who knows they have diabetes and understands how to recognise and treat hypoglycaemia. Also, it is important that people with diabetes never stop taking insulin to avoid hypoglycaemia while drinking.
Conclusion
While alcohol can be safely consumed in moderation by many people with diabetes, it carries additional risks including hypoglycaemia and a higher risk of development and progression of complications. It is imperative that clinicians and people with diabetes are appropriately educated about safe levels of alcohol consumption and practical strategies to avoid alcohol-related harm.
References
1.Australian Institute of Health and Welfare. Alcohol (AIHW): Overview [Internet]. Canberra, Australia; Australian Government; 2019 [updated 15 Jan 2018; cited 6 July 2019]. Available from: https://www.aihw.gov.au/reports-data/behaviours-risk-factors/alcohol/overview
2.Australian Bureau of Statistics (ABS): National Health Survey First Results 2017-18 [Internet]. Canberra, Australia; Australian Government; 2019 [updated 27 May 2019; cited 6 July 2019]. Available from: https://www.abs.gov.au/ausstats/abs@.nsf/PrimaryMainFeatures/4364.0.55.001?OpenDocument
3.
Baker IDI Health and Diabetes Institute: Diabetes â the silent pandemic and its impact on Australia [Internet]. Baulkham Hills, NSW, Australia; Novo Nordisk; 2012; [updated 2012; cited 6 July 2019]. Available from https://static.diabetesaustralia.com.au/s/fileassets/diabetes-australia/e7282521-472b-4313-b18e-be84c3d5d907.pdf
4.Lee CMY, Colagiuri R, Magliano D, Cameron A, Shaw J, Zimmet P et al. The cost of diabetes in adults in Australia. Diabetes Res Clin Prac [Internet]. 2013 [cited 6 July 2019]; 99(3): 385-90. Available from: doi: 10.1016/j.diabres.2012.12.002
5.Skyler JS, Bakris GL, Bonifacio E, Darsow T, Eckel RH, Groop L et al. Differentiation of Diabetes by Pathophysiology, Natural History and Prognosis. Diabetes [Internet]. 2017 Feb [cited 14 July 2019]; 66(2):241-255. Available from: https://doi.org/10.2337/db16-0806
6.Swade TF, Emanuele NV. Alcohol & diabetes. Compr Ther. 1997 Feb [cited 14 July 2019]; 23(2):135-140. Available from: http://europepmc.org/abstract/med/9083725
7.Ben G, Gnudi L, Maran A, Gigante A, Duner E, Lori E et al. Effects of chronic alcohol intake on carbohydrate and lipid metabolism in subjects with type II (non-insulin-dependent) diabetes. Am J Med [Internet]. 1991 [cited 6 July 2019]; 90:70-76. Available from: https://www.ncbi.nlm.nih.gov/pubmed/1986593
8.Arky RA, Freinkel N. Alcohol hypoglycaemia. Arch Intern Med [Internet]. 1964 [cited 6 July 2019]; 114(4):501-507. Available from: doi:10.1001/archinte.1964.03860100083009
9.Kerr D, Macdonald A, Heller SR, Tattersall RB. Alcohol causes hypoglycaemic unawareness in health volunteers and patients with Type 1 (insulin-dependent) diabetes. 1990 [cited 5 July 2019]; 33:216-221. Available from: https://www.ncbi.nlm.nih.gov/pubmed/2347435
10.Avogaro A, Beltramello P, Gnudi L, Valerio A, Miola M et al. Alcohol intake impairs glucose counterregulation during acute insulin-induced hypoglycaemia in IDDM patients: Evidence for a critical role of free fatty acids. Diabetes. 1993 [cited 5 July 2019]; 42:1626-1634. Available from: https://www.ncbi.nlm.nih.gov/pubmed/8405705
11.Arky RA, Veverbrants E, Abramson EA. Irreversible hypoglycaemia â a complication of alcohol and insulin. JAMA [Internet]. 1968 Oct [cited 14 July 2019]; 206:575-578. Available from: https://jamanetwork.com/journals/jama/article-abstract/341306
12.Day E, Rudd JHF. Alcohol use disorders and the heart. Addiction. 2019 Sep;114(9):1670-1678.
13.. Wakabayashi I. Inverse association of light-to-moderate alcohol drinking with cardiometabolic index in men with diabetes mellitus. Diabetes Metab Syndr. 2018 Nov;12(6):1013-1017.
14.Yeomens MR. Alcohol, appetite and energy balance: is alcohol intake a risk factor for obesity? Physiol Behav [Internet]. 2010 [cited 14 July 2019]; 100:92-9. Available from doi: 1016/j.physbeh.2010.01.012.
15.Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26 year follow-up of participants in the Framingham Heart Study. Circulation [Internet]. 1983 May [cited 14 July 2019]; 67(5):968-77. Available from: https://www.ncbi.nlm.nih.gov/pubmed/6219830
16.Kim SJ, Kim DJ. Alcoholism and Diabetes Mellitus. Diabetes Metab J [Internet]. 2017 Apr [cited 14 July 2019]; 36(2): 108-115. Available from doi: 4093/dmj.2012.36.2.108
17.Noor NM, Basavaraju K, Sharpstone D. Alcoholic ketoacidosis: a case report and review of the literature. Oxf Med Case Reports [Internet]. 2016 Mar [cited 11 Aug 2019] 2016(3):31-33. Available from doi:Â 10.1093/omcr/omw006
18.McGuire LC, Cruickshank AM, Munro PT. Alcoholic ketoacidosis. Emerg Med J [Internet]. 2006 [cited 14 July 2019]; 23(6):417-420. Available from doi: 1136/emj.2004.017590
19.Baranoa E, Lieber CS. Effects of ethanol on lipid metabolism. J Lipid Res [Internet]. 1979 Mar [cited 14 July 2019]; 20(3):289-315. Available from: https://www.ncbi.nlm.nih.gov/pubmed/87483
20.Lee JS, Chang PY, Zhang Y, Kizer JR, Best LG, Howard BV. Triglyceride and HDL-C Dyslipidemia and Risks of Coronary Heart Disease and Ischemic Stroke by Glycemic Dysregulation Status â The Strong Heart Study. Diabetes Care [Internet]. 2017 Apr [cited 14 July 2019]; 40():529-537. Available from: https://doi.org/10.2337/dc16-1958
21.Chait A, Macini M, February AW, Lewis B. Clinical and metabolic study of alcoholic hyperlipidaemia. Lancet [Internet]. 1972 July [cited 14 July 2019]; 62-64. Available from doi: 1016/s0140-6736(72)91552-8
22.Lin RC, Dai J, Lumeng L, Zhang MY. Serum low density lipoprotein of alcoholic patients is chemically modified in vivo and induces apolipoprotein E synthesis by macrophages. J Clin Invest [Internet]. 1995 May [cited 14 July 2019]; 95(5):1979-1986. Available from doi:Â 10.1172/JCI117882
23.O’Keefe E. L., DiNicolantonio J. J., O’Keefe J. H., Lavie C. J. Alcohol and CV health: Jekyll and Hyde Jâ Prog Cardiovasc Dis 2018; 61: 68â 75.
24.International Alliance for Responsible Drinking (IARD). Drinking and Liver Disease [Internet]. Washington DC; International Alliance for Responsible Drinking; 2017 [cited 11 Aug 2019]. Available from: http://www.iard.org/wp-content/uploads/2016/01/HR-Liver-Disease.pdf
25.Liangpunsakul S, Chalasani N. What do we recommend our patients with NAFLD about alcohol use? Am J Gastroenterol [Internet]. 2012 [cited 11 Aug 2019]; 107(7): 976-978. Available from doi:Â 10.1038/ajg.2012.20
26.Lodhi M, Amin J, Eswaran S. Role of alcohol in non-alcoholic steatohepatitis: Rush university (Con) patients with non-alcoholic steatohepatitis should be abstinent from alcohol use. Clinical Liver Disease â A multimedia review journal. 2018 [cited 11 Aug 2019]; 11(2): 39-42. Available from https://doi.org/10.1002/cld.669
27.McCulloch DK, Campbell IW, Prescott RJ, Clarke BF. Effect of alcohol intake on symptomatic peripheral neuropathy in diabetic men. Diabetes Care [Internet]. 1980 [cited 14 July 2019]; 3:245-247. Available from https://doi.org/10.2337/diacare.3.2.245
28.
Mitchell BD, Vinik A. Alcohol consumption â A risk factor for diabetic neuropathy? Diabetes [Internet]. 1987 [cited 14 July 2019]; 36 (Suppl. 1):71A
29.Sancho-Tello M, Muriach M, Barcia J, Bosch-Morell F, Genoves JM, Johnsen-Soriano S. Chronic alcohol feeding induces biochemical, histological, and functional alterations in rat retina. Alcohol and alcoholism [Internet]. 2008 [cited 14 July 2019]. 43(3):254-260. Available from: https://doi.org/10.1093/alcalc/agn006
30.Kohner EM, Aldington SJ, Stratton IM, Manley SE, Holman RR, Matthews DR. United Kingdom Prospective Diabetes Study, 30: Diabetic retinopathy at diagnosis of non-insulin dependent diabetes mellitus and associated risk factors. Arch Ophthalmol [Internet]. 1998 Mar [cited 14 July 2019]; 116(3):297-303. Available from: https://www.ncbi.nlm.nih.gov/pubmed/9514482
31.McCulloch DK, Young RJ, Prescott RJ, Campbell IW, Clarke BF. The natural history of impotence in diabetic men. Diabetologia [Internet]. 1984 [cited 14 July 2019]; 26:437-440. Available from: https://www.ncbi.nlm.nih.gov/pubmed/6468793
32.Grossman M. Low Testosterone in Men with Type 2 Diabetes: Significance and Treatment. J Clin Endocrinol Metab. 2011 Aug [cited 14 July 2019]; 96(8):2341-53. Available from: doi: 10.1210/jc.2011-0118
33.Muthusami KR, Chinnaswamy P. Effect of chronic alcoholism on male fertility hormones and semen quality. Fertil Steril [Internet]. 2005 Oct [cited 14 July 2019]; 84(4): 919-24. Available from: https://www.ncbi.nlm.nih.gov/pubmed/16213844
34.White ND. Alcohol Use in Young Adults With Type 1 Diabetes Mellitus. Am J Lifestyle Med [Internet]. 2017 [cited 11 Aug 2019]; 11(6): 433-435. Available from doi:Â 10.1177/1559827617722137
35.Weathermon R, Crabb D. Alcohol and Medication Interactions. Alcohol Res Health [Internet]. 1999 [cited 14 July 2019]; 23(1):40-54. Available from: https://pubs.niaaa.nih.gov/publications/arh23-1/40-54.pdf
36.Ahmed M, McKenna MJ, Crowley RK. Diabetic Ketoacidosis in Patients with type 2 Diabetes Recently Commenced on SGLT-2 Inhibitors: an ongoing concern. Endocr Pract. 2017;23(4):506-508.
37.Engler PA, Ramsey SE, Smith RJ. Alcohol use of diabetes patients: The need for assessment and intervention. Acta Diabetol. 2013 April [cited 14 July 2019]; 50(2):93-99. Available from: doi:10.1007/s00592-010-0200-x
38.Glasgow AM, Tynan D, Schwartz R, Hicks JM, Turek J, Driscol C et al. Alcohol and drug use in teenagers with diabetes mellitus. J Adolesc Health [Internet]. 1991 [cited 14 July 2019]; 12:11-14. Available from: https://www.jahonline.org/article/0197-0070(91)90033-I/fulltext
39.Cox WM, Blount JP, Crowe PA, Singh SP. Diabetic patientsâ alcohol use and quality of life: Relationships with prescribed treatment compliance among older males.
40.Karter AJ, Ferrara A, Darbinian JA, Ackerson LM, Selby JV. Self-monitoring of blood glucose. Diabetes Care. 2000 Apr [cited 14 July 2019]; 23(4):477-483. Available from: https://doi.org/10.2337/diacare.23.4.477
41.National Health and Medical Research Council (NHMRC) Australian guidelines to reduce health risks from drinking alcohol [Internet]. Canberra: NHMRC; 2009 9updated 3 December 2015; cited 14 July 2019]. Available from: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ds10-alcohol.pdf
42.National Diabetes Services Scheme. Alcohol [Internet]. Canberra: Diabetes Australia; June 2016 [cited 14 July 2019]. Available from: https://static.diabetesaustralia.com.au/s/fileassets/diabetes-australia/1efbdb03-be43-440f-b11d-e58a1ca3818d.pdf